Welcome to the first interactive and online EEG atlas!
We are excited to present a great collection of EEGs covering broad topics ranging from normal EEG findings to EEGs of rare syndromes.
Each EEG will present a short clinical vignette and a detailed report with interpretation. Additionally, many EEGs will have accompanying texts describing the most important findings and providing links to references for further reading.
Our goal is to provide a free and easily accessed atlas to anyone involved in this field, from neurologists to EEG technologists.
This atlas is compatible with Firefox, Chrome, Safari, and Edge browsers.
To use the Atlas please log in or Sign Up
This EEG atlas is based on the Cleveland Classification, developed by Professor Hans Lüders (Lüders and Noachtar, atlas and classification of electroencephalography, 2000). This classification allows for an objective description of the EEG that is reproducible, redundancy free, avoids subjective terms and correlates the electrographic findings to their clinical significance.
The structure of the EEG report contains the following components:
► Level of abnormality.
► EEG background description.
► Individual EEG findings description.
► Clinical interpretation of electrographic findings.
● Each EEG report starts by specifying the degree of abnormality based on the ictal and
interictal findings.
(Log in and click on any finding for detials)
● The background section describes the states in which the EEG is recorded including wakefulness, drowsiness, and/or sleep. This section documents the PDR and sleep structures as applicable.
● Findings in each EEG are then described individually in details including the type of
abnormality or finding, distribution, frequency and morphological description. Each
detail is documented using objective terms and avoids any subjective terms.
▸ For example, the frequency of a spike is described in Hz and not “frequent” or “rare”.
Similarly,
▸ the amplitude is described by voltage and not “low” or “high”.
● Using objective terminology ensures that the reader has an accurate impression of the EEG.
Furthermore, using objective description ensures reproducibility and allows for accurate
comparisons between different EEGs. This section is strictly dedicated to the
electrographic findings and contains no clinical correlation, which is documented at the
end of the EEG report.
By convention, the most prominent and important abnormality is classified first,
followed by the less severe ones.
▸ Epileptiform findings are classified first with ictal
▸ followed by interictal findings.
▸ Non-epileptiform findings are classified next starting with the more frequent and prominent
ones.
For example,
continuous focal sowing is classified before background slow.
Based on that, an EEG seizure pattern is classified first, followed by interictal findings and then
background slowing.
Such an order reflects the importance of these findings in clinical practice and avoids mixing
ictal
and interictal
findings.
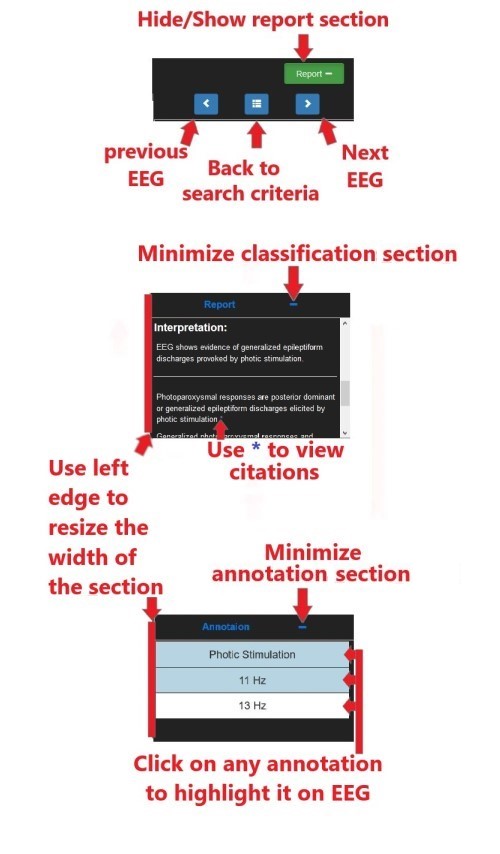
● The last part of the EEG report is the interpretation, which is describing the clinical significance of the electrographic findings in the previous section without describing the electrographic findings themselves. For example, an EEG seizure pattern classified above would be documented in terms of semiology and distribution (dialeptic, left temporal respectively) in the interpretation, but not in terms of the morphological details of the ictal pattern. This structure avoids repetition and redundancy, and mixing electrographic and clinical significance of the EEG.
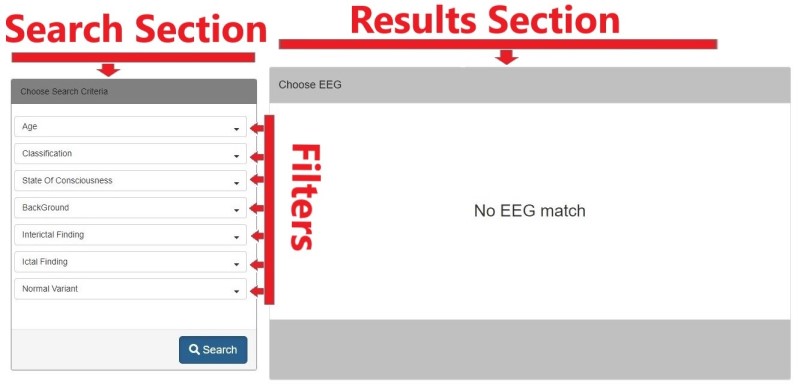
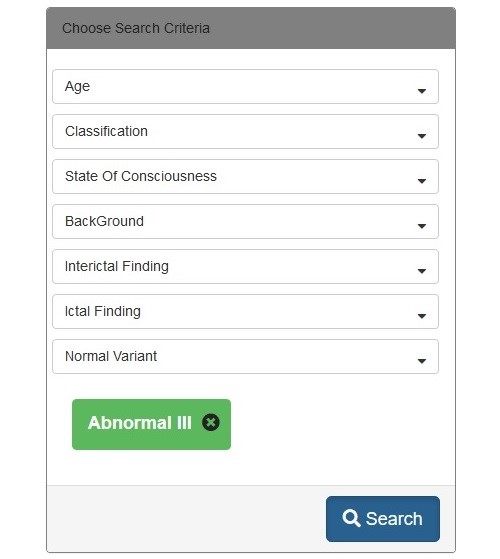
Use dropdown menus to build your search criteria
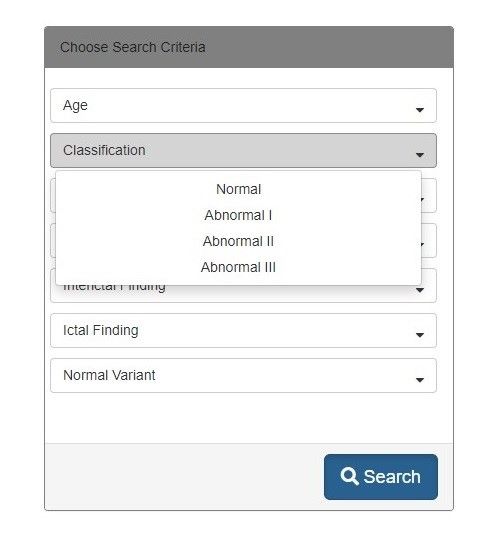
You can choose multiple criteria, narrow the criteria for more specific finding, or remove one of criteria.
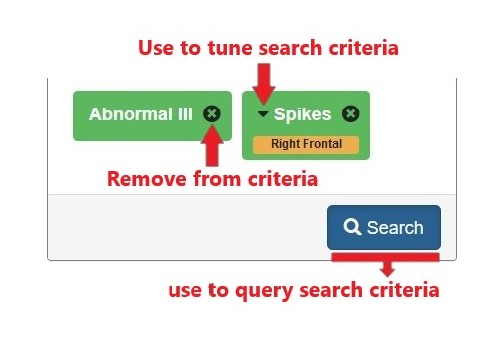
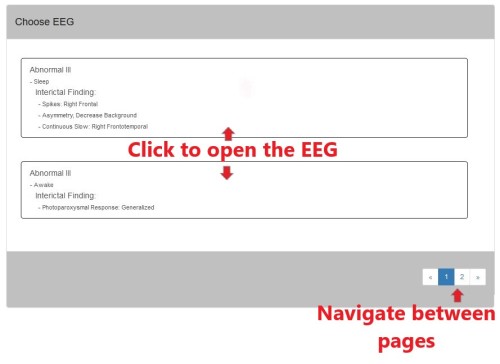
After quering search criteria, list of matching reports will populate the results section.


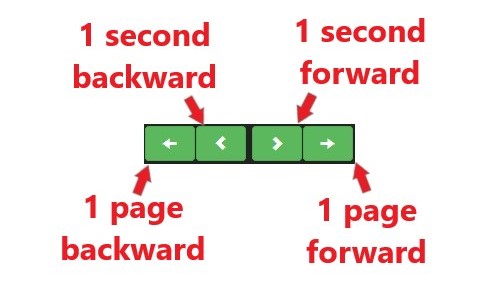
 change duration of the page.
change duration of the page.
 increase or decrease the amplitude.
increase or decrease the amplitude.
 apply filters, remove DC, 60 Hz notch, and/or 50 Hz notch.
apply filters, remove DC, 60 Hz notch, and/or 50 Hz notch.
Choose one of 6 standard montages as well as edit and create your own.

Montage 1:
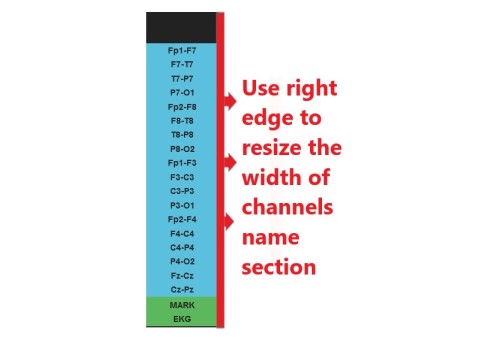
This is the classical bipolar, double banana montage with alternating left over right chains starting with the temporal then the parasagittal chains. Each chain is made of four channels except the central chain that is made of two channels.
Montage 2:
This is a referential montage with left hemispheric electrodes connected to the left ear electrode (A1) and right hemispheric electrodes connected to the right ear electrode (A2). This montage follows the convention of alternating left over right, temporal then parasagittal chains. Each chain is made of four channels. This montage is particularly useful for generalized epilepsies as well as focal epilepsies arising from or close to the midline.
Montage 3:
This is a bipolar montage that is made of alternating left over right channels. It contains the same channels of montage 1 but rearranged to allow comparison of homologous channels of the left vs right hemispheres as opposed to chains as in montage 1. This montage is useful to study asymmetries.
Montage 4:
This a referential montage to Cz with alternating left over right channels. It is most useful in temporal lobe epilepsy, or focal epilepsies arising far from the midline.
Montage 5:
This is a bipolar, circumferential montage with chains over the frontal, temporo-central and parieto-occipital regions. It is most useful for epilepsy arising from or near the midline.
Montage 6:
This is a bipolar montage that is a double banana montage with additional anterior temporal (FT9, FT10) or sphenoidal electrodes (Sp1, Sp2) added to the temporal chains. This montage is ideal for temporal lobe epilepsy.
enables to add, delete, or change order of channels in any montage.
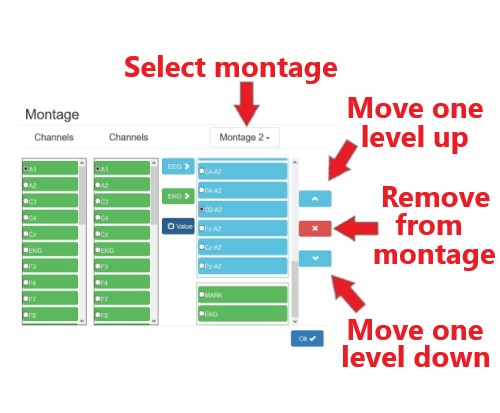
 add a new channel to the selected montage, the channel will be added to the bottom of the EEG.
Channel order
can be changed using order arrows.
add a new channel to the selected montage, the channel will be added to the bottom of the EEG.
Channel order
can be changed using order arrows.
 add a new channel to EKG.
add a new channel to EKG.
 enable/disable machine reference.
enable/disable machine reference.
The EEG Atlas is created by Bilal Zonjy, MD and Ahmad Marashly, MD.
This project is privately funded by Bilal Zonjy, MD and Ahmad Marashly, MD.
The software is created by Bilal Zonjy, MD.